1.C.7.a. Resident driven
Rule
Evidence that some rules are made by the residents that the residents (not the staff) implement.
Levels
|
I |
II |
III |
IV |
|
R |
R |
✔ |
✔ |
(✔ = required and R = recommended)
This standard rule is required for Level IIIs and Level IV recovery residences in order to mindfully ensure that the social model is being upheld despite the hierarchical staff model of the higher levels of support. Although Level Is and Level IIs more naturally uphold resident-driven governance, it is also recommended that they explicitly put a policy in place.
Guidance
Governance is about setting and enforcing boundaries. These are the rights, rules and decision-making procedures that direct actors (e.g. residents or staff) along a path that is desired. This rule speaks to resident-driven governance in which members of a community (e.g. residents, senior residents or alumni) develop and/or enforce boundaries, rules or decisions within or on behalf of the community. In the recovery housing world, this is often described as “peer accountability”. Too often the focus is on the enforcement side of resident-driven governance as opposed to the setting of rights, rules and decision making.
Understandably, some recovery residence providers worry that persons in early recovery may not have the skills to or a history of making “good” decision. Resident-driven governance is the opportunity for them to learn how to make “good” decisions for themselves and for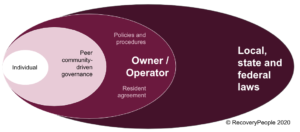 the community within the safety of external boundaries. Resident-driven governance happens within the boundaries of the external governance such as recovery residence policies and procedures, fidelity standards or local, state and federal laws.
the community within the safety of external boundaries. Resident-driven governance happens within the boundaries of the external governance such as recovery residence policies and procedures, fidelity standards or local, state and federal laws.
Social model recovery philosophy expects external governance structures to cultivate resident-driven governance within the recovery residence. The result is a cultural shift amongst residents from “Us vs Them” to “This is our community”.
Note: this rule is slightly different from standard rule 1.C.7.e. Resident Voices, which points to the external governance structure creating a process to consider and adopt ideas generated through community-driven governance.
Evaluation
- Is there evidence that residents can create rules or make decisions?
- Are these rules or decision implemented by resident(s)?
Evidence
- Policy and procedure
- Staffing and governance plan
- Interview: “How does your recovery residence create opportunities for community-driven governance? What are examples of rules that resident(s) have created and enforced? Or some decisions residents have made?
Resource
Culture, Structure and Accountability in Recovery Housing (RecoveryPeople.org)